ACL Reconstruction Surgery India at affordable cost
What Is The Anterior Cruciate Ligament?The anterior cruciate ligament (ACL) is one of the most important of four strong ligaments connecting the bones of the knee joint. It is often injured.
Ligaments are strong, dense structures made of connective tissue that stabilize a joint. They connect bone to bone across the joint.
Get ACL Knee Surgery treatment that help for Injured Knees... and ACL Knee Surgery in India possible in cheap cost
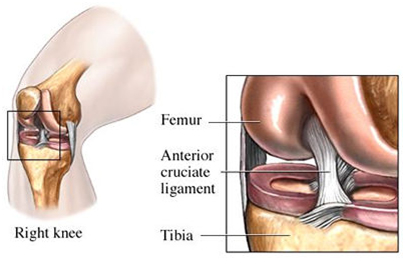
- It restrains excessive forward movement of the lower leg bone (the tibia) in relation to the thigh bone (the femur).
- It limits rotational movements of the knee.
A tear to the anterior cruciate ligament (ACL) results from overstretching of this ligament within the knee.
- It's usually due to a sudden stop and twisting motion of the knee, or a force or "blow" to the front of the knee.
- The extent of the tear can be a partial or a complete tear.
- Individuals experiencing a tear to the ACL may or may not feel a pop at the time of the injury.
- It is often injured together with other structures inside the knee joint.
- After the initial injury, the knee may swell and become painful.
- Instability or a sensation the knee is "giving out" may be a major complaint following this injury.
Often, but not always, depending on a person's activity level, a torn ACL needs to be fixed. Unfortunately a simple repair by suturing the torn ligament together again is not effective. A successful repair involves completely replacing the torn ligaments, and there are a number ways that this can be done.
Understanding The Knee
The knee is a hinge joint made up of three bones held firmly together by ligaments that stabilize the joint. The bones that meet at the knee are the upper leg bone (the femur), the lower leg bone (the tibia), and the knee cap (the patella). A smooth protective layer called cartilage which allows the bones to glide smoothly upon each other, lines the bones inside the joint. In arthritis, this smooth lining becomes damaged.Ligaments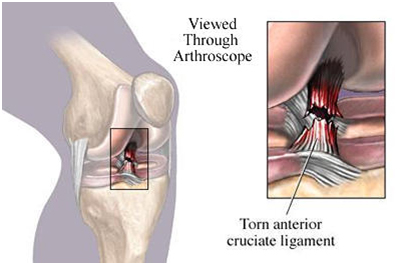
Ligaments are dense structures of connective tissue that fasten bone to bone and stabilize the knee. Inside the knee joint are two major ligaments : -
- The anterior cruciate ligament (ACL)
- The posterior cruciate ligament (PCL)
These cross in the center of the knee (that's why they're called cruciate ligaments -a crucifix is a cross). They control the backward and forward motion of the knee. The ACL in particular restrains excessive forward motion of the knee as well as the inward twisting or rotation of the knee. The ACL is frequently injured in severe twisting injuries of the knee.
Two other major ligaments are actually located outside the knee joint, on the outer and inner side of the knee. They act to stabilize the knee's sideways motion. The ligament on the inner side of the knee is called the medial collateral ligament (MCL) (medial means inner side). The ligament on the outer side of the knee is the lateral collateral ligament (LCL) (lateral means outer side).
The patellar tendon (the 'ligament' of the knee cap) connects the lower part of the kneecap (patella) to the upper part of the tibia , specifically to the lump one can feel just below the knee on the lower leg bone (the tibia). Part of this tendon is commonly used in reconstructing a torn ACL.
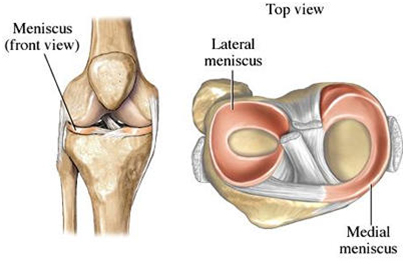
Meniscus
The meniscus is a half-moon-shaped structure placed between the weight-bearing bone ends in the knee. There are two menisci in each knee, one on the inner side called the "medial meniscus" and one on the outer side called the "lateral meniscus."
- The two menisci act as shock absorbers within the knee and also help spread the weight load.
- The meniscus is a type of cartilage, though it is different than the cartilage that lines the bones.
- The menisci may be torn during twisting movements of the knee. A meniscus is frequently torn at the same time an ACL tears during injury.
Muscles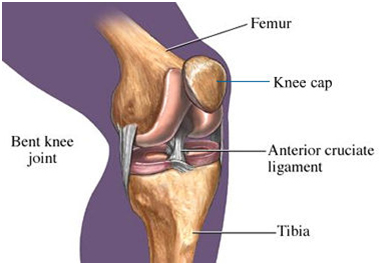
Muscles control the movement of the knee joint. Rehabilitation of these muscles is most important following an ACL injury or reconstruction. The major muscles of the knee joint involved with bending and straightening the knee are : -
Quadriceps
The quadriceps muscle is made up of the four large muscles at the front of the thigh (these muscles are the rectus femoris, the vastus lateralis, the vastus intermedius, and the vastus medialis). Together they form a large fleshy mass covering the front and sides of the thigh bone. This is the main muscle group that straightens the knee (called extension of the knee).
Hamstrings
The hamstring muscles are the muscles at the back of the upper leg. They flex (bend backward) the lower leg. Individually, the muscles of the hamstrings are the biceps femoris, semitendinosus, and semimembranosus.The biceps femoris is a large muscle comprised of two heads called the long head and short head, converging to a single tendon as it inserts below the knee joint. This common tendon is located on the outer back corner of the knee and forms the outer hamstring. Another member of the hamstring muscles is the semitendinosus muscle originating from the back of the pelvis and crossing below the back of the knee joint. This muscle, along with the tendon from another hamstring muscle called the semimembranosus and yet another inner groin muscle called the gracilis muscle, form the inner hamstring.
Tendons are tough tissues that connect the muscles to the bone. The hamstring tendons are frequently used in reconstruction of the ACL.
Facts About Anterior Cruciate Ligament Tears : -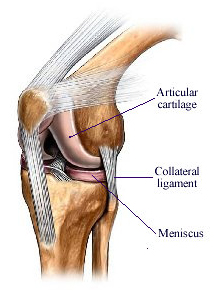
- The anterior cruciate ligament (ACL) provides almost 90% of the stability to the knee joint.
- More than 11.2 million visits are made to physicians' offices because of a knee problem. It is the most often treated anatomical site by orthopedic surgeons.
- Of the four major ligaments in the knee, the anterior cruciate ligament and the medial collateral ligament are most often injured in sports.
- Reconstruction of a torn ACL is now a common procedure, with over 50,000 hospital admissions per year.
- ACL ruptures occur at a rate of 60 per 100,000 people per year. With society's increasing interest in physical fitness, primary care physicians are seeing more athletic injuries. Along with these injuries are the commonly experienced ACL ruptures in athletes and non-athletes alike. Today's athletes have greater than a 90% chance of returning to their pre-injury level of sports participation.
- ACL reconstruction is a highly successful operation. With good rehabilitation, 90% to 95% of individuals who undergo this surgery can expect to return to full sports participation within six months.
What Causes An ACL Tear?
Movements of the knee that place a great strain on the ACL can cause damage to the ligament.
- Hyperextension of the knee, that is, if the knee is straightened more than 10 degrees beyond its normal fully straightened position, is a very common cause of an ACL tear. This position of the knee forces the lower leg excessively forward in relation to the upper leg.
- Pivoting injuries of the knee with excessive inward turning of the lower leg can also damage the ACL.
Basically any athletic or non-athletic related activity in which the knee is forced into hyperextension and/or internal rotation may result in an ACL tear.
Activities placing the knee into hyperextension and /or the tibia into excessive inward rotation can be from either an outside force or non-contact in nature.
The severity of the injury to the knee will depend on : -
- The position of the knee at the time of the injury.
- The direction of the blow.
- The force of the blow.
Most ACL injuries occur during athletic activity. Often those are non-contact activities with the mechanism of injury usually involving : -
- Planting and cutting - the foot is positioned firmly on the ground followed by the leg (and body for that matter) turning one direction or the other. Example: Football or baseball player making a fast cut and changing direction.
- Straight-knee landing - results when the foot strikes the ground with the knee straight. Example: Basketball player coming down after a jump shot or the gymnast landing on a dismount.
- One-step-stop landing with the knee hyperextended - results when the leg abruptly stops while in an over-straightened position. Example: Baseball player sliding into a base with the knee hyperextended with additional force upon hyperextension.
- Pivoting and sudden deceleration resulting from a combination of rapid slowing down and a plant and twist of the foot placing extreme rotation at the knee. Example: Football or soccer player quickly slowing down followed by a quick turn in direction.
About 40% of all individuals experience a "popping" sensation at the time of the injury, which is actually the tearing of the ligament tissue. At least half of all anterior ligament tears also cause injury to one of the menisci of the joint, which may also produce a tearing sensation.
Hyperextension (forceful over-straightening) is most often caused by accidents associated with : -
- Skiing
- Volleyball
- Basketball
- Soccer
- Football
Because the ACL becomes taut with inward rotation of the tibia, activities placing any excessive inward rotation of the tibia (usually seen from a plant and twist mechanism) are seen in sports such as : -
- Football
- Tennis
- Basketball
- Soccer
Injury to the ACL may occur in other sports such as : -
- Wrestling
- Gymnastics
- Martial arts
- Running
Non-Athletic-Related Injuries
Non-sport related injuries to the ACL result from similar contact and non-contact stresses on the ligament. Examples vary from being struck on the outer side of the knee to landing on the knee forcing it into an over-straightened position with the knee turned inward.Motor vehicle accidents in which the knee is forced under the dashboard may also cause rupture of the ACL.
Repeated trauma and wear and tear can be a knee problem at any age causing small tears in the ligament, which over time become complete tears.
Diagnosing An ACL Tear
The diagnosis of an ACL tear is based on
- The physician's examination, as well as special tests which may include
- Radiographic Evaluation.
- MRI (Magnetic Resonance Imaging).
- KT 1000.
Physical Examination
The physician will take a thorough history addressing how the injury occurred and ascertaining when the pain may have first appeared. Questions regarding any earlier knee injuries are important as often ligaments and cartilage structures may have been previously strained. Any previous episodes of knee instability or the knee giving way is important information.
The physician can determine the integrity of the ACL by conducting special ligament stability tests. One simple but important test is called the Lachmans test. With the knee bent to 30 degrees, the physician gently pulls on the tibia to check the forward motion of the lower leg in relation to the upper leg. A normal knee will have less than two to four mm of forward movement, with a firm stopping felt when no further movement is observed. In contrast, a knee with an ACL tear will have increased forward motion and a soft end feel at the end of the movement. This is because of the loss of restraint of the forward movement of the tibia due to the torn ACL.
A similar test, with the knee bent to 90 degrees, is called the anterior drawer test. A more complex test is called the pivot shift test, in which greater stresses are put on the knee as it is straightened by the physician from a bent and inwardly rotated position. If the knee "gives," this is an indication that other stabilizing structures inside the knee must be torn besides the ACL. This test can sometimes only be done when the knee is completely relaxed. Because of this it may best be observed under anesthesia during the surgical procedure.
Radiographic Evaluation
Acute knee injuries generally warrant x-ray films. They are carefully evaluated for any possible tearing away of bone where the ligaments attach. Also, the x-ray will show any loose bone fragments or other fractures if they are present.MRI
Magnetic resonance imaging is a noninvasive test that produces an excellent image of all parts of the knee. In this test, the individual lies in a hollow cylinder while powerful magnets create signals from inside the knee. These signals are then converted into a computer image that clearly shows any damage to the structures inside the joint. The images are valuable not only to determine the presence of an ACL tear, but also the degree of the tear along with any damage to related structures, such as the meniscus and other ligaments.
KT 1000 
An instrument called the KT 1000 is a device that can give information about the integrity of the ACL. It allows the doctor or therapist to measure the amount of forward motion of the lower leg in relation to the upper leg. It is used frequently. Both knees are usually tested and then compared. This device also accurately measures the amount of backward movement of the knee joint.
What Can Be Done For An ACL Tear?
The initial goals of treatment immediately after injury are to reduce pain and swelling and regain range of motion and strength. Even if surgery is likely, achieving as much knee motion and strength as possible can greatly reduce complications after surgery.
Immediately After The injury
Immediately after an ACL injury, the so-called R.I.C.E. treatment is recommended.R.I.C.E. stands for : -
- Rest : - The individual is advised to rest the knee from weight-bearing activities allowing the swelling to settle.
- Ice : - Placing a cold compress or ice pack on the knee is helpful in controlling inflammation as well as helping to reduce pain.
- Compression : - Utilizing an ace wrap for compression around the knee is beneficial to control the swelling.
- Elevation : - Lying down with the leg elevated higher than the level of the chest is helpful in controlling and reducing swelling.
The physician may request very gradual weight-bearing exercise immediately after the initial ACL injury. Braces used early after the injury are called rehabilitation kneebraces and are off-the-shelf designs used for conservative treatment of the ligament tear. This type of brace is also used for postoperative care of the injured ACL. The rehabilitation brace, also called a post-operative brace, is used immediately post-injury in an effort to put the joint at rest and help protect it, while still allowing appropriate but limited motion.
This form of bracing is available in two particular types : -
- Straight immobilizer : - Made of foam with two metal rods down the side that is secured with Velcro and prevents all motion.
- Hinged brace : - Allows range of motion to be set by tightening a screw control.
Post-Injury Exercises
As the swelling in and around the joint decreases and weight-bearing progresses, mild strengthening exercises are started.
Quadriceps sets are one example of strengthening exercises at this stage. With the knee placed at approximately 10 degrees from being straight, along with a small towel roll directly behind the knee, the individual pushes downward into the towel roll for a count of six to 10 seconds. This is repeated 10 times. It should be done several times throughout the day.
Increasing the range of motion of the knee becomes a very important part of the program to avoid joint stiffness and muscle tightness. Sliding the heel of the injured leg towards the buttock until a gentle stretch is felt is also a good exercise. This stretch is held for 10 to 20 seconds and is repeated 10 times, several times a day.
Bracing
Bracing for the anterior cruciate ligament comes in two forms : -
- Rehabilitation Brace
- Functional Brace
Functional or sport braces are available both off-the-shelf and as custom-fit. Physicians prescribe this type of brace to treat the unstable knee in people when surgery is not recommended, as well as to protect the knee in those who have had surgery. Functional braces can be worn as the individual returns to work, training, or competition. But they may be most beneficial for individuals who have some instability and who place low to moderate stress loads upon the knee.
It is important to the individual who does have instability of the knee from an ACL tear that functional knee braces will guarantee against instability in activities that require cutting, pivoting, or other quick changes in direction. A well-fitting brace will not restrict normal knee movement.
Do I Have To Have Surgery ?
Treatment decisions for ACL tears are always individualized - tailored to each individual. The decision whether to offer surgery is based on the person's age, activity level, how unstable the knee is, and whether other structures in the knee have been injured.
It is important to keep in mind that surgery to reconstruct a torn ACL is not an emergency for most people. Many people with a torn ACL do not need surgery at all. Even though the chances for complete success from surgery are now excellent, surgery is not for everyone. This is because not everyone needs the ligament repaired to return to his or her pre-injury level of function.
It is important to distinguish whether the work, recreational, and athletic activities of the person is light, moderate, or strenuous. Another important issue that needs to be understood by the individual considering ACL reconstruction is that it requires many weeks and months of hard work in rehabilitation following the reconstruction. This needs commitment and time.
The Ultimate Deciding Factors...
- Whether the injury is a recent tear or an old ACL problem, individuals need to consider their present activity level and decide if their daily activities and livelihood would be affected by the injury. The question of whether to have surgery to reconstruct the torn ACL arises most frequently with less athletically inclined older persons. Generally in such people, if the instability is severe, and the knee is constantly buckling, the decision to offer surgery is intended to prevent further damage to the knee and stop the daily discomfort of the knee giving way.
- On the other hand, if the knee instability can be controlled by avoiding activities that the individual doesn't really mind avoiding, then going the "conservative" route and avoiding surgery is often a very good choice - and many people are satisfied with it. Certainly, there are many older athletes who are willing to avoid basketball, soccer, or racquetball, and stick to jogging or biking for fitness. As long as their knees are stable and pain-free for these activities, they are happy. Also with the use of a functional brace, many of these people find they can do most of what they wish to do without significant problems.
- For those people who choose not to have surgery, this does not mean going without any treatment at all. There is still a treatment program to be followed emphasizing strengthening the leg muscles and learning to better control the knee and to avoid those situations most likely to cause instability. Many people benefit from this kind of rehabilitation.
- If athletics is a regular part of your life, or if your work is likely to be affected by mild instability of the knee (for example, construction workers or other non-sedentary type jobs), your physician will lean toward reconstructing the torn ligament.
- In general, stronger and fitter is better - and this applies to operated and non-operated knees equally.
Reconstruction Surgery For ACL Tears
If it has been decided that you are a candidate for surgery it is important to be both mentally and physically prepared. This includes understanding the injury, the surgery, and the rehabilitation goals.
How is the ACL repaired?
Preparing For Surgery
The initial goals before surgery are to : -
- Reduce swelling in the knee.
- Get back the normal range of motion of the knee.
- Walk normally. This may take anywhere from one week to as long as two months depending on how the knee responds to the initial injury).
Depending on your age, certain preoperative tests will be arranged, such as blood tests, urine tests, chest x-ray, and an EKG.
Leg measurements may be taken to order a knee brace. Your rehabilitation program will be discussed in detail with you.
You will meet the anesthesiologist, who may offer you a choice of anesthesia:
- If you choose a general anesthetic, you will be asleep during the procedure.
- If you choose an spinal, an injection is given into the back that numbs the lower half of the body. This wears off a couple of hours after surgery.
If you have an spinal anesthetic, you can often watch the whole operation on the television monitor.
Need to Know : -
- If you take aspirin, anti-inflammatory drugs, or blood thinners, you should stop taking them one week before surgery to minimize bleeding. Discuss this with your doctor.
- You should not eat or drink anything (even water) for six hours before surgery. This usually means not eating or drinking anything after midnight the night before surgery.
- If you would normally be taking medication during the hours before surgery, talk to your doctor.
Need to Know : -
What to tell your doctor ?Be sure to tell your doctor : -
- If you are allergic to iodine or any other drugs.
- What medications you take.
- About your past medical history.
- If you've ever had deep vein thrombosis or other blood clotting abnormalities.
Also tell your doctor if you develop any of these symptoms prior to surgery : -
- Fever or chills.
- Irritation of the eyes, ears, throat or gums.
- Sniffling or sore throat.
- Boils or inflamed skin abrasions and cuts
How Is The ACL Repaired?
There are a number of different techniques available to repair a torn ACL. Each surgeon has his preference for each particular situation.
In fact we don't talk about ACL "repair" but rather about ACL "reconstruction." This is because a torn ACL cannot simply be repaired by sewing it together again. This was the method tried in the early days of repairing ACL tears, but it was shown to be ineffective. Thus, newer methods were developed which involve reconstructing the ACL ligament, including substituting a new ligament for the damaged one. Using tendons from other parts of the body as a substitute for the ACL was found to be the most effective way of reconstructing the torn ACL. Currently, the two most popular methods in use are using part of the patella tendon or using a hamstring muscle tendon.
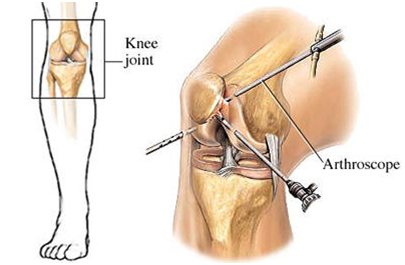
Today ACL reconstruction is essentially an arthroscopic procedure, though many surgeons throughout the world still prefer to open the knee. If this route is chosen, depending on how the ACL is repaired, then the incisions may not be very different from those done arthroscopically
An arthroscope is a pen-shaped instrument to which a tiny video camera is attached. It contains optical fibers, a light source, and lenses that can magnify images 25 to 30 times. The camera attached to the end of the arthroscope sends images to a video screen. The surgeon looks at the screen and is able to get an exceptionally clear view of the inside of the joint. Because the procedure can be done using an arthroscope, and using small specialized instruments without big incisions and excessive trauma to the tissues, it is really well suited to be an outpatient procedure (one that does not require an overnight stay at the hospital). Most ACL reconstructions are commonly performed as outpatient procedures. However, many doctors prefer to keep patients overnight in the hospital following surgery.
Before actually reconstructing the torn ligament, the surgeon uses the arthroscope to carefully survey the whole joint, looking at and evaluating each key structure. During this portion of the procedure, any additional damage to any of the other knee structures can be identified, and where appropriate, is corrected surgically.
There are a number of choices available to the orthopedic surgeon in determining how best to reconstruct the torn ACL. They all involve a "graft" using something to substitute for the torn ACL.
Each of the available ACL graft tissue choices requires a unique harvesting technique. Furthermore, there are usually different methods used for fixing the grafts in the bone tunnels, depending on the characteristics and properties of the tissue selected. Because of these differences in graft techniques, the type of surgery chosen is frequently made by the surgeon based on his or her experience and comfort level with the chosen technique.
Typically, an ACL reconstruction takes two to two and a half hours. The anesthesia may be general anesthesia or a spinal anesthesia. General anesthesia allows the individual to be asleep through the entire procedure. Spinal anesthesia involves an injection in the back that numbs only the lower body. A medication is also administered with a spinal anesthesia to keep the individual sedated throughout the procedure.
There are several available operative procedures : -
Patellar tendon graft procedure
Since it was popularized in the mid-1980s, the patellar tendon graft has been the "gold standard" choice for ACL reconstruction. This type of ACL replacement uses the middle third of the person's own patella tendon and is referred to as a bone-tendon-bone (BTB) graft.
In this particular technique
- Two tiny incisions for arthroscopic instruments are usually placed on either side of the patellar tendon.
- A one- to two-inch incision is made over the patellar tendon on the front of the knee and the tendon is exposed. The middle one-third of the patellar tendon is carefully removed, together with two bits of bone on either end (hence it is called a 'bone-tendon-bone graft').
- Two small tunnels are then drilled into the bones on either side of the joint, in the area where the torn ACL normally attaches to the bone, to allow for fixation of the new ligament.
- The patellar tendon graft is then passed into the joint, placed in a position similar to the original ACL, with the bone pieces at each the end of the graft fitting nicely into the tunnels that have been drilled in the bone.
- The new ACL is then secured with a specialized headless screw in each tunnel. The patellar tendon graft is tightly secured at the time of the surgery. The knee is stable enough to begin motion and weight-bearing as tolerated, as per the surgeon's instructions.
As healing occurs, the bone tunnels fill in to further secure the tendon ends of the graft in a bone-to-bone relationship. This occurs over the next six to eight weeks.
Nice to Know : -
Recent technology has led to the development of specialized absorbable screws that actually dissolve within the bone over two to three years.Advantages : -
- The fixation is very strong
- The patellar tendon replacing the ACL is as strong as the injured ACL (or even stronger).
- A few people have mild discomfort on the front of the knee, especially when kneeling. This generally settles down within a year. Workers who kneel frequently may need to look at other graft options.
- A normal patellar tendon has been altered. However, this does heal fully again.
Hamstring graft procedure
Hamstring reconstruction is an alternative to the bone-patellar-bone graft fixation and is growing in popularity. In this procedure, rather than using the patellar tendon, the surgeon uses the patient's own hamstring tendon, either the semitendinosus or gracilis tendons from the same leg.There are several variations of this technique. Newer hamstring fixation techniques have been developed to match and even exceed the initial pullout strength of the patellar tendon bone procedure described above. Special screws with threads designed not to cut the hamstring tendons are able to fix the tendon within the bone tunnel, as described with the patellar tendon bone technique.
In younger patients who have torn their ACLs but still have growing bones, the hamstring tendon graft is a good choice because there is less chance of damaging the 'growth plates'- the area responsible for growth of the bone.
Advantages : -
- The hamstring incision is away from the patella, allowing patients to kneel comfortably.
- The patellar tendon is left intact.
Disadvantages ; -
- Soft tissue-to-bone healing occurs at a slower rate than bone-to-bone healing.
- Unlike the patellar tendon, the hamstring tendons do not grow back after graft harvest resulting in a slight loss in hamstring strength (approximately. average of 10%) after recovery. However, most people do not notice this slight decline in strength.
Allograft procedure
Another option is the use of tissue from a cadaver (a deceased person) called an allograft.Patellar tendon, hamstring tendon, or Achilles tendon allografts can be used as tissues inserted and fixed with the same techniques that are used for autografts (grafts using the individual's own tissue).
Allografts are a good choice when the patient's own tissue availability is limited. They are useful for complicated ligament reconstructions needing more than one graft (for example, if both anterior and posterior cruciate ligaments need to be replaced) or if both the ACL and patellar tendon are damaged.
Advantages : -
-
. No risks, pain, or scars from the donor site . Operative time is quicker
- The very low risk of contracting a serious infection from the cadaver tissue. Newer techniques of tissue radiation have minimized this risk.
- National shortage of allografts due to a high demand combined with a low supply of suitable, qualified cadavers.
Nice to Know : -
Synthetic grafts
Synthetic grafts (i.e., grafts made from other materials) were commonly used in the 1970s but were generally unsuccessful.There are currently no synthetic ligaments in the U.S. approved by the FDA for primary ACL reconstruction.
Researchers continue to try and create the perfect ACL replacement. Major requirements of a prosthetic ligament are that it must be strong, matching the compliance of a normal ACL. It must be durable, withstanding high repetitive loads without wear. It also must be perfectly tolerable to the host without bone, joint, or systemic reaction
What Can I Expect After My ACL Reconstruction?
For most individuals with a torn ACL, reconstruction will restore stability to the knee. Reconstructed knees are reliable and stable. The knee will not give out unexpectedly and will allow the person to return to previous work and athletic activities, usually without any compromises.
A protective brace is often recommended for athletic activities.
Approximately 90% of individuals return to their previous level of activity without restrictions. For the competitive athlete, this can be extremely important. In some cases, it is even a matter of earning a living or funding a college education. In the case of non-athletes, it can be equally as important in returning to their pre-injury level on and off the job.
Nice To Know : -
Q: What kind of brace will I be using when I return to my sport after rehabilitation?A: There are several types of braces on the market that protect the knee joint. They are all relatively light and user friendly. One important aspect some ACL braces have is that in order to unload stress on the ACL graft, the sequence of fastening the straps of the brace (usually four or five) is very important.
Q: I like to snow and water ski. Can I still do these activities after ACL reconstruction?
A: Unless the surgeon advises otherwise, most people return to enjoying both of these sports with the use of a brace. However, remember every individual injury is different. Following the recommendations of the surgeon is of utmost importance.
The list of of Knee Joint Replacement Hospitals in India is as follows : -
- Apollo Hospitals, Bangalore, India
- Apollo Hospital, Chennai, India
- Apollo Hospitals, Hyderabad, India
- Indraprastha Apollo Hospital, Delhi, India
- Apollo Gleneagles Hospital, Kolkata, India
- Apollo Hospital, Goa, India
- Wockhardt Hospital, Bangalore India
- Wockhardt Hospital, hyderabad, India
- Wockhardt Hospital, Mumbai, India
- BGS Global Hospital, Chennai, India
- Fortis Hospital, Delhi, India
- Fortis Hospital, Mohali, India
- Fortis Hospital, Noida, India
- Manipal Hospital, Bangalore, India
- BGS Global Hospital, Hyderabad, India
- MIOT Hospital, Chennai, India
- Sparsh Hospital, Bangalore, India
- Artemis Hospital, Gurgaon ( Delhi ) , India
- Max Devki Devi Heart and Vascular hospital, Delhi, India
- BGS Global Hospital, Bangalore, India
For more information, medical assessment and medical quote send your detailed medical history and medical reports as email attachment to Email : - info@wecareindia.com Call: +91 9029304141 (10 am. To 8 pm. IST) (Only for international patients seeking treatment in India)
We Care Health Services Hospitals






Copyright © 2009 - 2015 We Care India. All Rights Reserved.
Home | About Us | Site Map | Get a Quote | Disclaimer | Advertise With Us | Contact Us